ParentVibes
Women's Health Library · parentvibes.in
Female Fertility: Causes of Difficulty Conceiving, Tests & Treatment Options
Quick Facts
Female fertility is the ability to conceive and carry a pregnancy. It depends on several things working together — regular ovulation, healthy fallopian tubes and uterus, and balanced hormones. For many women everything works smoothly; for others, one or more factors can make conceiving harder. Either way, understanding how it works — and what can be done — is empowering.
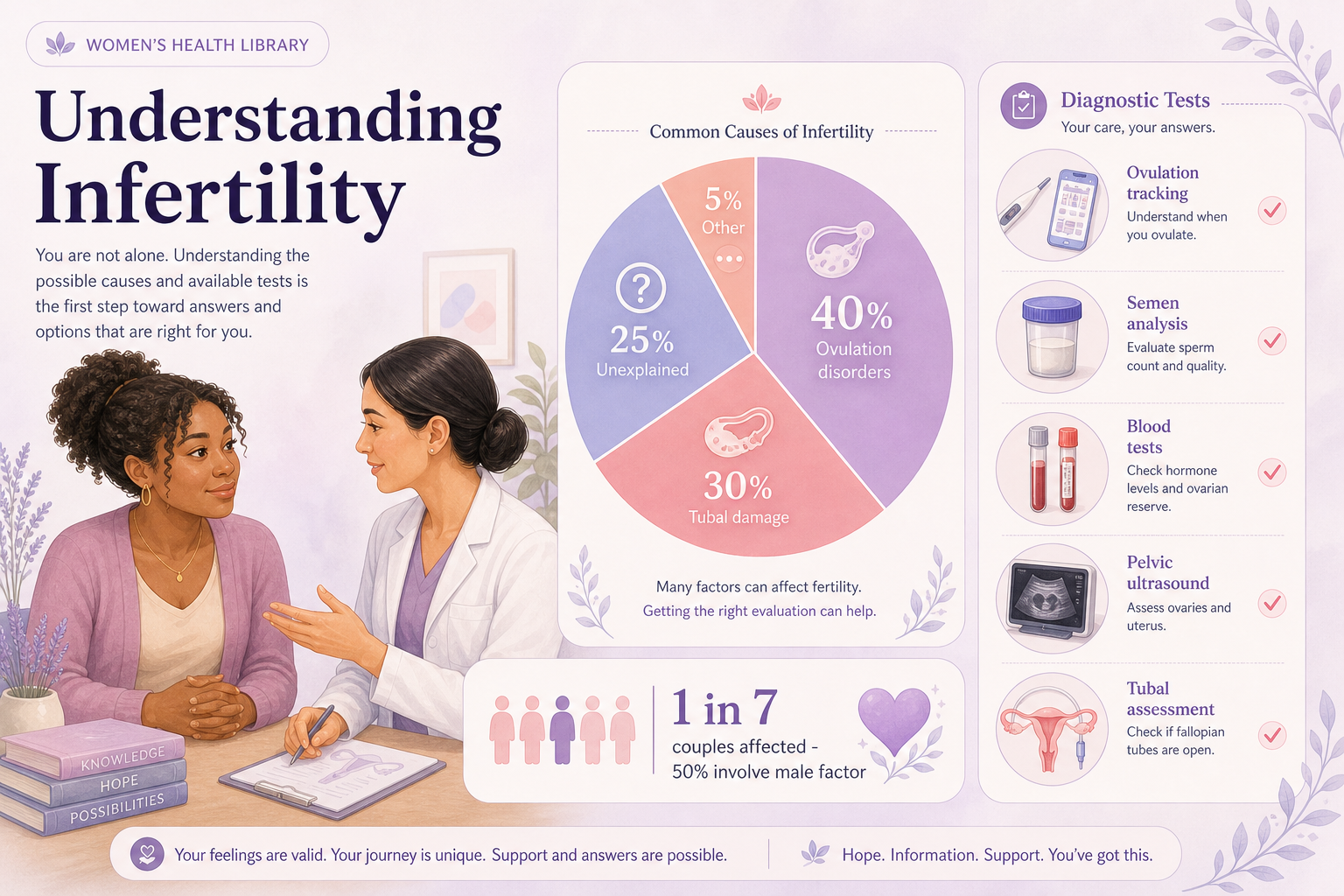
Worldwide, around 1 in 6 people of reproductive age experience infertility at some point, and it affects men and women roughly equally. In women, the most common causes of difficulty conceiving are problems with ovulation, blocked or damaged fallopian tubes, endometriosis, and age-related changes. Importantly, many of these are treatable, and a great many women go on to conceive with the right support.
This guide explains the common causes, the tests doctors use, and the treatment options — always with the message that you deserve compassionate, expert care. Difficulty conceiving is common and not a personal failing.
Bring data to your doctor
Tracking cycles and ovulation in ParentVibes gives your specialist a valuable head start.
Open the tracker →Useful tools
Things worth knowing
Conception is a chain of events
An egg must release, travel an open tube, meet sperm, and implant in the uterus.
It's not just a woman's issue
Infertility affects men and women roughly equally, so the partner is always assessed.
Ovulation problems are a leading cause
Conditions like PCOS, thyroid issues and high prolactin are common — and often treatable.
Age is the biggest natural influence
Fertility declines from the mid-30s and more steeply after 40 — normal biology, not effort.
Testing clarifies the picture
No symptoms doesn't rule out a cause; tests look for the cause in both partners.
It is never a personal failing
Difficulty conceiving is common, and many women conceive with the right support.
Everything You Need to Know (How Fertility Works & Age)
Conception requires a chain of events: an egg matures and is released (ovulation), travels through an open fallopian tube, meets healthy sperm, and the resulting embryo implants in a receptive uterus. A problem anywhere along this chain can affect fertility.
| Factor | Why it matters |
|---|---|
| Ovulation | No egg released = no conception; ovulation problems (e.g. PCOS) are a leading cause |
| Fallopian tubes | Must be open for egg and sperm to meet; blockage (often from past infection) prevents this |
| Uterus | Fibroids, polyps or shape issues can affect implantation |
| Egg quantity & quality (ovarian reserve) | Decline with age, especially after the mid-30s |
| Age | The single biggest natural influence on female fertility |
About age
Female fertility gradually declines with age and falls more noticeably from the mid-30s, with a steeper decline after 40. This is normal biology — not a reflection of health or effort — and is why earlier evaluation is advised for women over 35.
Signs
Often there are no obvious symptoms beyond difficulty conceiving — but some signs point to specific causes:
Signs that may point to a cause
- Irregular or absent periods — may indicate ovulation problems (e.g. PCOS, thyroid)
- Very painful periods or pain during sex — may suggest endometriosis
- Heavy bleeding — may relate to fibroids
- History of pelvic infection/STI — may suggest tubal damage
- Hormonal signs — excess hair, acne (PCOS); milky discharge (prolactin)
Track while you read
Tick the symptoms that apply to you. This is a self-check, not a diagnosis — saved on this device only.
Absence of symptoms doesn't mean absence of a cause — and presence of one doesn't guarantee a problem. Testing clarifies.
Causes
Common causes of female difficulty conceiving:
- Ovulation disorders
- Including PCOS, thyroid problems, and high prolactin (a very common, often treatable cause).
- Tubal factors
- Blocked/damaged fallopian tubes, often following past pelvic infection (e.g. untreated STIs).
- Endometriosis
- Tissue similar to the womb lining growing elsewhere, affecting fertility and causing pain.
- Uterine factors
- Fibroids, polyps, adhesions, or structural differences.
- Age-related decline
- Reduced egg quantity and quality over time.
- Unexplained infertility
- No clear cause found despite testing (still often treatable).
- Male factor
- Present in a large share of couples, so the partner is always assessed.
Fertility Testing
A fertility evaluation looks for the cause in both partners. Timing: after 12 months of trying, 6 months if the woman is 35+, and promptly if 40+ or there are known risk factors.
Female tests may include
- Ovulation confirmation — a progesterone blood test ~7 days before the expected period
- Hormone tests — thyroid, prolactin, and ovarian-reserve markers (e.g. AMH, FSH)
- Tubal & uterine checks — an HSG (tubal X-ray) or specialised ultrasound (HyCoSy), and sometimes laparoscopy/hysteroscopy
- Pelvic ultrasound — for ovaries, follicle count, fibroids, etc.
- Male test: a semen analysis — always part of the workup
Keep all results in ParentVibes Medical Records to share across appointments.
Treatment
Treatment depends on the cause, age and circumstances — and there are many effective options:
- Ovulation problems (e.g. PCOS)
- Lifestyle measures; ovulation-inducing medicines (letrozole/clomifene).
- Mild/unexplained
- Lifestyle; IUI in some cases.
- Blocked tubes / endometriosis / complex
- IVF or surgery in selected cases.
- Male factor
- Treat the cause; ICSI with IVF.
- Age-related
- Timely specialist input; IVF; (where relevant) donor options.
Track your plan
The ParentVibes IVF Dashboard helps you and your clinic track tests, medicines and cycles together.
Open IVF Dashboard →Specialist care only
Fertility medicines and procedures are prescription-only and require monitoring (e.g. to avoid over-stimulation). A fertility specialist creates a plan tailored to you.
Supporting Your Fertility
Lifestyle won't fix every cause, but it genuinely supports fertility and treatment success:
Fertility-supportive habits
- Healthy weight — both very low and very high weight affect ovulation and outcomes
- Balanced diet + folic acid
- Stop smoking; limit alcohol and excess caffeine
- Regular moderate exercise — avoid extremes that disrupt cycles
- Manage stress — fertility journeys are hard; support helps wellbeing
- Track ovulation and time intercourse across the fertile window
When to See a Doctor
See a fertility specialist (with your partner) if:
- You've tried for 12 months without success (under 35)
- You've tried for 6 months and are 35+
- You're 40+ — seek advice promptly
- You have irregular/absent periods, PCOS, endometriosis, or a history of pelvic infection/surgery
- You've had recurrent miscarriage or previous fertility issues
- You simply want a fertility check or have concerns
Use Ask a Doctor on ParentVibes, or book a fertility review via Doctor Visits & Appointments.
Continue learning
Frequently Asked Questions
What are the most common causes of female infertility?
Ovulation problems (like PCOS), blocked fallopian tubes, endometriosis, uterine issues, and age-related decline.
At what age does female fertility decline?
It gradually declines with age, more noticeably from the mid-30s and more steeply after 40.
What fertility tests will I have?
Often ovulation/hormone blood tests, ovarian-reserve markers, tubal checks (HSG), and a pelvic ultrasound — plus a semen analysis for your partner.
Can female infertility be treated?
Yes — many causes respond to lifestyle measures, ovulation medicines, surgery, or assisted reproduction like IVF/IUI.
Does PCOS mean I can't get pregnant?
No — PCOS affects ovulation but is a common, treatable cause; many women with PCOS conceive.
Is infertility the woman's fault?
No. It affects men and women roughly equally, often involves both partners, and is never a personal failing.
When should we get tested?
After 12 months of trying, 6 months if you're 35+, or promptly if 40+ or there are known issues.
Was this guide helpful?
Understand your cycle better with ParentVibes
- Track your period dates
- Predict your next cycle
- Understand your fertile window
- Save health notes
- Get gentle reminders
Related tools
Period Tracker
Log periods and learn your personal cycle pattern.
Open tool
Ovulation Calculator
Estimate your ovulation date and fertile window.
Open tool
Fertility Window
See your most fertile days for trying to conceive.
Open toolPregnancy Tracker
Follow your pregnancy week by week once you conceive.
Open tool
Due Date Calculator
Estimate your baby's due date from your last period.
Open toolShare this guide with someone who needs it 💛
Medical review
- Last reviewed
- June 2026
- Medical reviewer
- Dr. Vinika G.
- Next review due
- June 2027
- Status
- Medically reviewed by Dr. Vinika G.
References
This article is for general information and education only and is not a substitute for professional medical advice, diagnosis, or treatment. Fertility is individual and often involves both partners. Consult a qualified doctor or fertility specialist for assessment and before any treatment or medicine. In a medical emergency, contact your doctor or local emergency services immediately. Content reviewed against guidance from WHO, ACOG, NHS and peer-reviewed literature.
Planning Parenthood Library journey
100%Related guides
Free resources
Medical disclaimer
This article is for educational purposes only and does not replace medical advice. If you have severe pain, heavy bleeding, missed periods, or unusual symptoms, please consult a qualified healthcare provider.